Overview
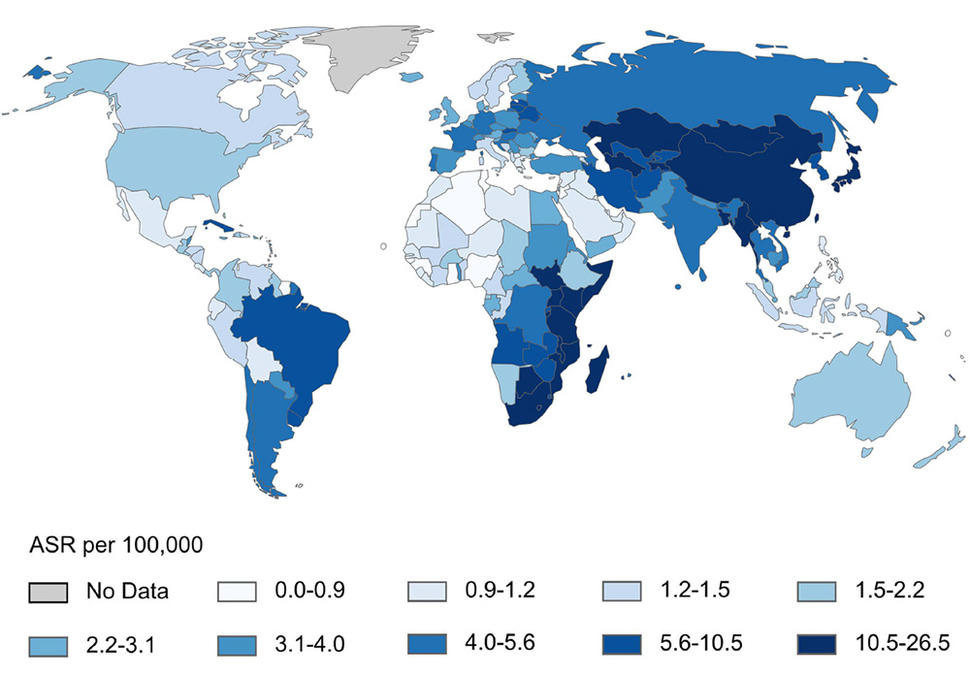
Incidence of esophageal squamous cell carcinoma (age standardized rates, per 100,000) for males.
Esophageal cancer is the seventh most common cause of cancer worldwide and the sixth most common cause of cancer-related death worldwide. Esophageal cancer kills 400,000 people every year, most of whom live in two distinct geographic bands across central Asia and along the eastern Africa corridor extending from Ethiopia to South Africa. In these high-risk areas, nearly all cases are esophageal squamous cell carcinoma (ESCC).
ESCC symptoms, such as dysphagia (difficulty swallowing) and weight loss, develop late. Most patients present with advanced disease, and survival is usually poor (3-6 months). Afflicted patients are readily identifiable in surgical and medical hospital wards, profoundly wasted and holding spittoon cups to manage secretions.
NCI investigators and others have performed many etiologic, genetic, early detection, and treatment studies of ESCC in central Asia, but this disease remains essentially unstudied in East Africa. To address this research gap, NCI and others have created the African Esophageal Cancer Consortium (AfrECC) which supports fieldwork and case-control studies in different settings in East Africa.
AfrECC Collaborating Centers
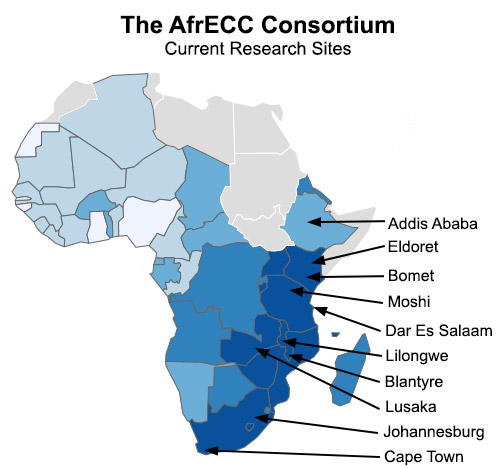
Over the past few years, African Esophageal Cancer Consortium (AfrECC) members have begun quality studies, in collaborating centers:
- Addis Ababa, Ethiopia (IARC and Addis Ababa University)
- Eldoret, Kenya (IARC and Moi University)
- Bomet, Kenya (NCI and Tenwek Hospital)
- Moshi, Tanzania (IARC and Kilimanjaro Christian Medical Center)
- Dar es Salaam, Tanzania (UCSF and Muhimbili University)
- Lilongwe, Malawi (NCI and the UNC-Malawi Project)
- Blantyre, Malawi (IARC and Queen Elizabeth Central Hospital)
- Lusaka, Zambia (University Teaching Hospital and Queen Mary University of London)
- Johannesburg and Cape Town, South Africa (University of the Witwatersrand and University of Cape Town)
Consortium Objectives
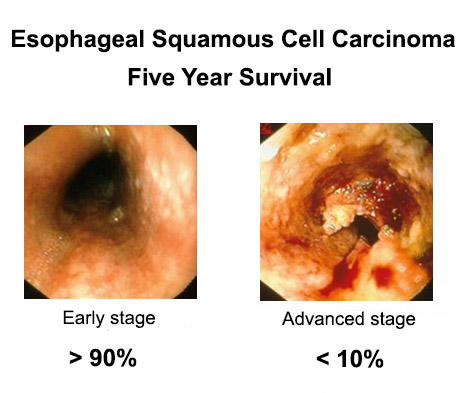
Five year survival for esophageal squamous cell carcinoma is dramatically different depending on the stage of disease.
Research
To coordinate etiologic and molecular studies of ESCC in this high-risk population:
- Data are being collected using an mHealth application tailored to the consortium, which increases efficiency, eliminates transcription mistakes, and allows real-time QC and supervision of field activities from any location.
- Unified data entry on mobile devices instantly harmonizes data and facilitates an internationally-coordinated effort.
- Case-control studies are in various stages of implementation at institutions in collaboration with the Oesophageal Squamous Cell Carcinoma African Prevention Research (ESCCAPE).
- Case-control studies will examine the etiological effects of dietary, lifestyle, and environmental risk factors for ESCC.
- Future molecular and genomic research is also planned, including a coordinated GWAS study.
Clinical Capacity Building

Ethiopian endoscopists learning esophageal stent placement.
To improve outcomes for early detection, treatment, and palliation of this cancer:
- The consortium established an in-region training center to teach stent placement and other endoscopic and surgical skills with the support of the American Society for Gastrointestinal Endoscopy.
- An important priority at all sites is provision of self-expanding metal stents (SEMS) for ESCC palliation. The consortium is actively working with international partners to provide affordable stents in Africa.
- Studies are being conducted exploring secondary prevention strategies through screening for the asymptomatic precursor lesion, esophageal squamous dysplasia (ESD).
- Central coordination is encouraging sites to learn from one another and spread technical research expertise.
- Biospecimen procedures and tumor biobanks are being standardized.
- A survey of regional endoscopy capacity is being conducted.

Endoscopists learning about esophageal stents.

Ethiopian endoscopists receiving esophageal dilator sets.

Ethiopian gastroenterology fellows graduating from their fellowship program.
Advocacy and Awareness
To raise awareness (both in Africa and elsewhere) of the importance of ESCC for physicians, at-risk populations, and policymakers:
- Education among at-risk populations and physicians to promote earlier presentations for clinical care, earlier diagnosis, and referrals to centers equipped to provide the necessary treatment or palliation.
- Advocacy for local ministries of health and international funding agencies is critical for the provision of resources to increase access to relevant therapies and to support the necessary research to drive development of evidence-based policies for prevention and palliation.
AfrECC Steering Committee

AfrECC Etiology Group meeting in Moshi, Tanzania in January 2023.
AfrECC Steering Committee members and their current terms include:
- Valerie McCormack (2024-2028)
- Geoffrey Buckle (2024-2028)
- Gift Mulima (2024-2028)
- Blandina Mmbaga (2022-2026)
- Violet Kayamba (2022-2026)
- Beatrice Mushi (2022-2026)
- Mark Topazian (2022-2026)
AfrECC Working Group Leads
Etiology Working Group co-chairs: Hannah Simba, Yukiko Yano
Clinical Working Group co-chairs: Lucien Ferndale, Yona Ringo
Remote Mentoring Working Group co-chairs: Jerry Waye, Alan Barkun
AfrECC Countries
- Botswana
- Brazil
- Cameroon
- Canada
- Djibouti
- Ethiopia
- France
- France/Botswana
- France/Zimbabwe
- Ghana
- Kenya
- Malawi
- Mozambique
- Rwanda
- South Africa
- Tanzania
- Uganda
- United Kingdom
- United States
- Zambia
- Zimbabwe
Membership Documents
AfrECC Virtual Meetings
AfrECC General Membership Meetings
AfrECC Steering Committee Meetings
AfrECC Etiology Working Group Meetings
AfrECC Clinical Working Group Meetings
Most meetings meet quarterly. Please visit https://africaecc.org/ for current schedule.
AfrECC Publications and Contact Information
Browse updated AfrECC Publications (pdf, 182KB).
For more information, please visit https://africaecc.org/