Overview
People with HIV have a higher risk of certain types of cancer, because HIV infection weakens the immune system, and because many other cancer risk factors are common among people with HIV. Investigators at the NCI seek to understand better the role of the immune system and certain infections in the development of cancer. Understanding patterns of cancer occurrence in the population of people with HIV may help identify important opportunities for cancer prevention.
Study Team
Drs. Eric Engels, Meredith Shiels, and Qianlai Luo
Eric A. Engels, M.D., M.P.H. – Co-principal investigator
Meredith S. Shiels, Ph.D., M.H.S. - Co-principal investigator
Qianlai Luo, Ph.D. – Staff scientist and study coordinator
Collaborators
Background and Purpose
The HIV/AIDS Cancer Match Study (HACM) is an observational study of over 850,000 people with HIV across multiple regions of the United States. One of the largest studies of cancer in people with HIV, the HACM Study is a long-standing collaboration between the National Cancer Institute (NCI) and state health departments. The study uses public health surveillance information on people with HIV and cancer, both of which are notifiable conditions to health departments. Health departments merge their disease-specific registries to construct a new database resource through which to study cancer risk among people with HIV.
The HACM Study focuses on the modern era of effective antiretroviral therapy starting in 1996 through the present time. The study has made important contributions to public health, including characterizing trends in cancer risk over the course of the entire HIV epidemic, understanding shifts in the projected cancer burden among aging populations on long-term antiretroviral therapy, and describing disparities in treatment and outcomes following a cancer diagnosis.
Note: This study does not recruit patients, and all identifiable information is removed from files used by researchers at NCI.
Study Design
The HACM Study is based on a series of computerized linkages between the databases (termed “registries”) that are maintained by state public health authorities. The NCI receives only anonymized data from these registries. NCI researchers use these study data to determine the spectrum of cancers that occur in people with HIV. The risk of cancer in people with HIV is compared with that in the general population to determine which cancers arise more frequently than expected. Investigators compare different groups of people with HIV, to determine whether certain individuals are at especially high risk of cancer. Through frequent updates of the data, investigators also monitor changing trends in cancer risk over time. Read more information on the study design and analytic practices in the HACM Study.
Study Sites
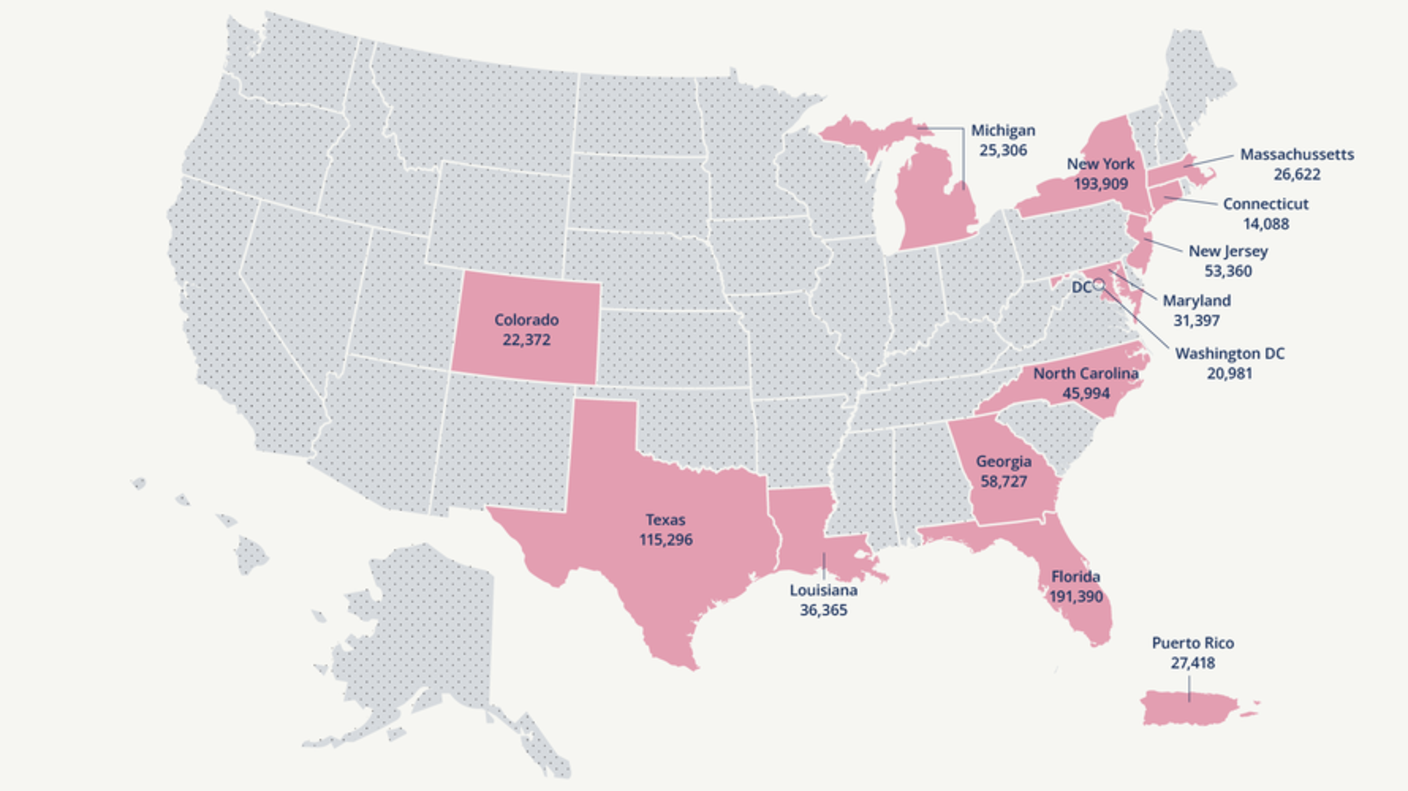
The HACM Study utilizes anonymized data provided by HIV and cancer registries in the United States. The map in Figure 1 below illustrates the regions that participate in the study, along with the number of people in the region with HIV that are included in the study. More detailed information is found in Table 1.
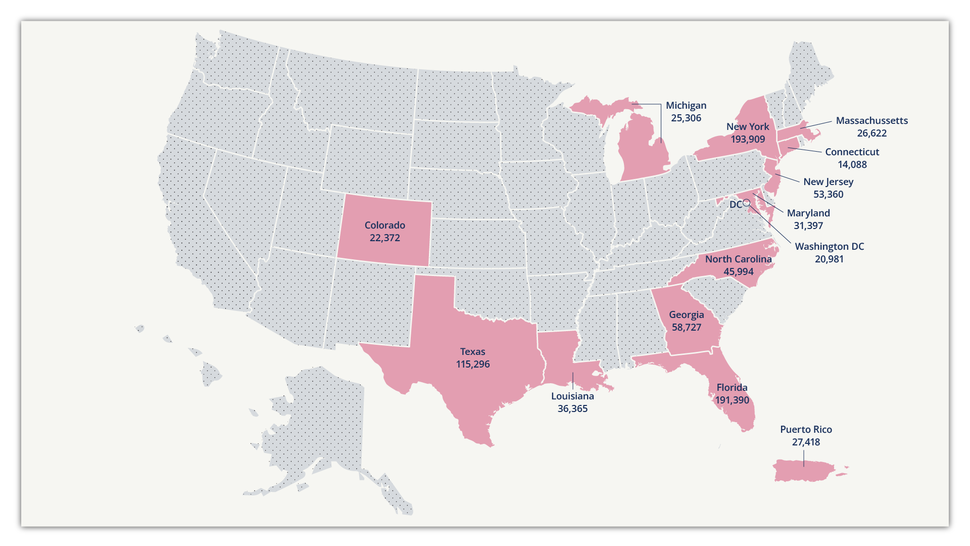
Figure 1. Regions that participate in the study, and the numbers of people with HIV that are included in the HACM study. More details (including calendar years and cancer cases) appear in Table 1.
| Region | Calendar Years | People with HIV | Cancers |
|---|---|---|---|
| Colorado |
1998–2015 | 18,252 | 1,720 |
| Connecticut |
2002–2016 | 14,088 | 2,030 |
| Washington, DC |
2007–2015 | 20,981 | 1,526 |
| Florida |
1997–2019 | 191,390 | 22,518 |
| Georgia |
2004–2012 | 58,727 | 2,658 |
| Louisiana |
1996–2015 | 36,365 | 2,860 |
| Massachusetts |
2007–2016 | 26,622 | 2,109 |
| Maryland |
2008–2018 | 31,397 | 2,537 |
| Michigan |
1996–2015 | 25,306 | 2,987 |
| North Carolina |
1996–2014 | 45,994 | 3,212 |
| New Jersey |
1996–2012 | 53,360 | 5,616 |
| New York |
2001–2019 | 193,909 | 26,450 |
| Puerto Rico |
2003–2017 | 27,418 | 1,881 |
| Texas |
1999–2019 | 139,714 | 8,636 |
| All Regions |
1996–2019 | 883,523 | 86,740 |
Higher Risk of Cancer Among People with HIV
People with HIV have a high risk of developing certain types of cancers, including Kaposi sarcoma, non-Hodgkin lymphoma, and cancers of the cervix, lung, liver, and anus. This high risk occurs because HIV weakens the immune system. Also, people with HIV frequently have other cancer-causing viruses at the same time. Tobacco and alcohol use increase the risk of certain cancer types. Selected cancers for which people with HIV have an elevated risk include:
- Kaposi sarcoma (KS): This cancer is caused by KS-associated herpesvirus, also known as human herpesvirus 8. Effective antiretroviral therapy (ART) reduces the risk of this cancer.
- Non-Hodgkin lymphoma (NHL): In many cases, this cancer is caused by Epstein-Barr virus. ART reduces the risk of this cancer.
- Cervical cancer: This cancer is caused by human papillomavirus. Women with HIV should receive regular screening for cervical cancer from their HIV provider or a gynecologist. Screening consists of a pelvic exam, during which the provider obtains a Pap smear and testing for high-risk strains of human papillomavirus. Screening can detect early stages in the development of cancer, which can be treated to prevent progression. Vaccination against human papillomavirus prevents infection.
- Lung cancer: This cancer is caused by smoking, which is very common in some HIV populations. People with HIV appear to be especially susceptible to the cancer-causing effects of tobacco. People with HIV should work with their healthcare provider to quit smoking. Medications and counseling can increase the chances of successfully quitting tobacco use. Individuals should also discuss the possible benefits of screening for lung cancer using low-dose computed tomography (CT) scanning, which is recommended for long-time smokers in the general population.
- Anal cancer: This cancer is caused by human papillomavirus. People who have had anal intercourse are at especially high risk, but the cancer can also occur among other groups of people with HIV.
- Liver cancer: This cancer is caused by infection with hepatitis B virus (HBV) and hepatitis C virus (HCV), and also by excessive alcohol intake and obesity. People with HIV should receive the HBV vaccine, if they have not already been infected with HBV. Treatment for HBV and HCV can result in suppression or clearance of these viruses. People with HIV who also have HBV or HCV infection should be monitored for liver damage and should moderate their use of alcohol.
Cancers for which people with HIV do not have an elevated risk are colon cancer, breast cancer, and prostate cancer. These cancers are common in the general population, and people with HIV do not have an increased risk compared with people who do not have HIV. Because effective therapy now allows people with HIV to live longer healthier lives, they should receive the same screening for these cancers as people in the general population.
Cancer Sites
| Cancer Type | N (Numbers) | % of Total |
|---|---|---|
| Kaposi sarcoma | 8,843 | 10.1 |
| Non-Hodgkin lymphoma | 14,538 | 16.7 |
| Cervix | 3,416 | 3.9 |
| Lung | 7,177 | 8.2 |
| Prostate | 5,750 | 6.6 |
| Anal | 10,613 | 12.2 |
| Liver | 2,707 | 13.1 |
| Hodgkin lymphoma | 2,794 | 3.2 |
| Female breast | 3,484 | 4.0 |
| Colon | 1,989 | 2.3 |
| Other | 25,822 | 29.6 |
| Total | 87,133 | 100.0 |
Study Results and Select Publications
The HIV/AIDS Cancer Match Study provided important advances in our understanding of cancer risk among people living with HIV. Initially, this cohort allowed investigators to describe the enormous increase in risk for cancers associated with immunosuppression early in the AIDS epidemic and later the marked declines in these AIDS-defining malignancies with the introduction of effective antiretroviral therapy.
The study documented a strongly increased risk for a rare skin cancer, Merkel cell carcinoma, which led other investigators to the eventual discovery of a novel cancer virus, Merkel cell polyomavirus.
Today, study teams are describing the contemporary risks of people with HIV as they age and with the introduction of new preventive measures, like the HPV vaccine. They have characterized the spectrum of cancer risk in people with HIV, identified risk factors for cancer in this population, and evaluated survival outcomes following a cancer diagnosis. These findings have helped clarify the role of immunosuppression in shaping cancer incidence and survival. The results have also been important for understanding the overall burden of cancer in the US HIV population.
Select Publications
- Research Highlight: Cancer Treatment Disparities Persist for People with HIV
- Severe anal intraepithelial neoplasia trends and subsequent invasive anal cancer in the United States
- Cumulative incidence of anal cancer since HIV or AIDS diagnosis in the United States
- Survival by sex and HIV status in patients with anal cancer in the USA between 2001 and 2019: a retrospective cohort study
- Risk of Liver Cancer Declines for People with HIV, But Rates Remains Elevated
- Trends and risk of lung cancer among people living with HIV
- Impact of HIV on anal squamous cell carcinoma rates
- Years of life lost to cancer among the HIV population
- Kaposi sarcoma incidence, burden, and prevalence in people with HIV
- Deaths attributable to cancer in the United States HIV population
- Projected Cancer Incidence Rates and Burden among HIV-Infected Adults
Browse the list of all HIV/AIDS Cancer Match Study publications.
Collaboration and Data Sharing
The HIV/AIDS Cancer Match Study data provide a valuable resource for cancer epidemiology research. Study data are used for the following purposes:
- Identify cancers that occur at increased frequency in people with HIV.
- Describe changes in cancer burden over time, which may reflect changes in HIV therapy, demographic characteristics such as aging, or other factors.
- Describe the spectrum of cancer in subgroups of people with HIV of particular interest.
- Identify associations with markers of HIV infection status (such as CD4 count and HIV viral load).
- Focus on specific cancers (including rare cancers) to identify the effects of immunosuppression and other demographic and medical factors that may reflect etiology.
- Identify predictors of cancer outcome.
- Provide information for the National Cancer Institute and other policy making bodies on the impact of HIV on cancer risk and trends in morbidity and mortality over time.
Ideas for specific projects and collaborations related to these aims are welcome. The HIV/AIDS Cancer Match Study principal investigators are the custodians for the data. Agreements between the NCI and participating registries do not allow the NCI to share the data with external investigators. Also, the study data are complex and require the use of sophisticated data handling and statistical modeling techniques. Collaborators can use the study data at the NCI under close supervision by the principal investigators or can participate in analyses through review of tabulated data.
Interested collaborators should contact the HIV/AIDS Cancer Match Study principal investigators:
- Eric A. Engels, M.D., M.P.H. – Co-principal investigator
- Meredith S. Shiels, Ph.D., M.H.S. – Co-principal investigator